|
Clinical Image
An anomalous optic nerve
1 University of California, Irvine School of Medicine, Irvine, California 92697, USA
2 Gavin Herbert Eye Institute, Department of Ophthalmology, UC Irvine, California 92697, USA
3 Department of Biomedical Engineering, UC Irvine, California 92697, USA
4 Beckman Laser Institute and Medical Clinic, UC Irvine, California 92697, USA
Address correspondence to:
John Abdelmalek
University of California, Irvine, 850 Health Sciences Road, Irvine, CA 92697-4375,
USA
Message to Corresponding Author
Article ID: 100053Z17JA2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Abdelmalek J, Malley CE, Browne AW, Ediriwickrema LS. An anomalous optic nerve. J Case Rep Images Opthalmol 2026;9(1):15–17.ABSTRACT
No Abstract
Keywords: Optic nerve, Retinal schisis, Vitreopapillary traction
Case Report
An 80-year-old woman with hypertension, hyperlipidemia, asthma, and breast cancer requiring lumpectomy and radiation was referred for an ophthalmic examination after experiencing acute onset blurry vision in the left eye for six months. The patient also reported monocular diplopia described as “overlapping shadows” in the left eye.
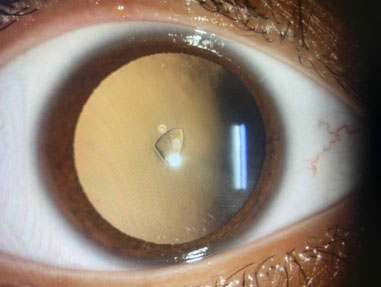
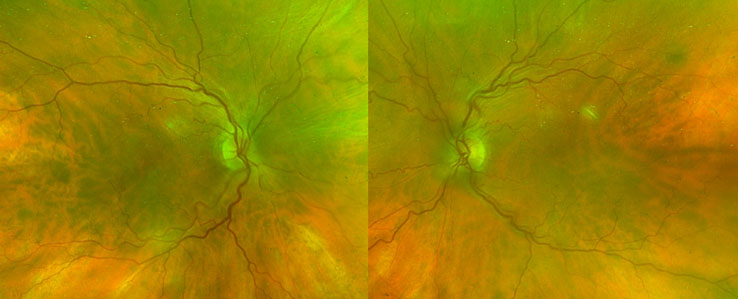
Best correct visual acuity at the time of presentation was 20/20 in the right eye and 20/40 in the left eye, with the patient reporting subjective improvement in her affected eye since onset of symptoms. Humphrey visual field testing showed non-specific changes in the right eye and no notable findings in the left eye, and was reliable with minimal fixation losses, false positives, and false negatives. Color vision was normal (24/24 OU on Hardy-Rand-Rittler Pseudoisochromatic color plate testing under monocular conditions). Anterior segment evaluation revealed symmetrical nuclear sclerotic cataracts in both eyes. Fundus examination identified a mildly hyperemic left optic nerve and vascular tortuosity in both eyes with cup-to-disc ratios at 0.05 bilaterally (Figure 1). Schisis without subretinal fluid was noted alongside the peripapillary retina. The remainder of the dilated fundus exam was reassuring.
Upon further questioning, the patient reported spending several weeks at 9000 feet elevation approximately around the time of symptomatic onset, developing an upper respiratory viral illness two months prior, and traveling aboard a cruise ship one month prior.
Discussion
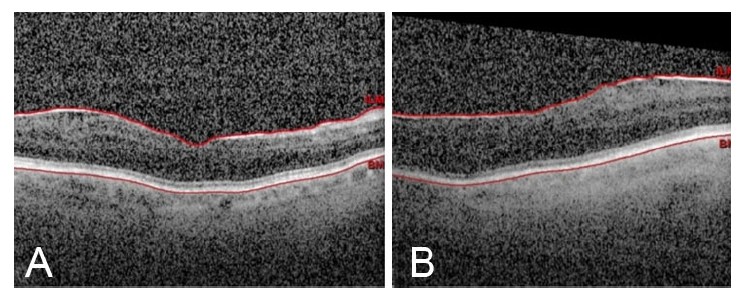
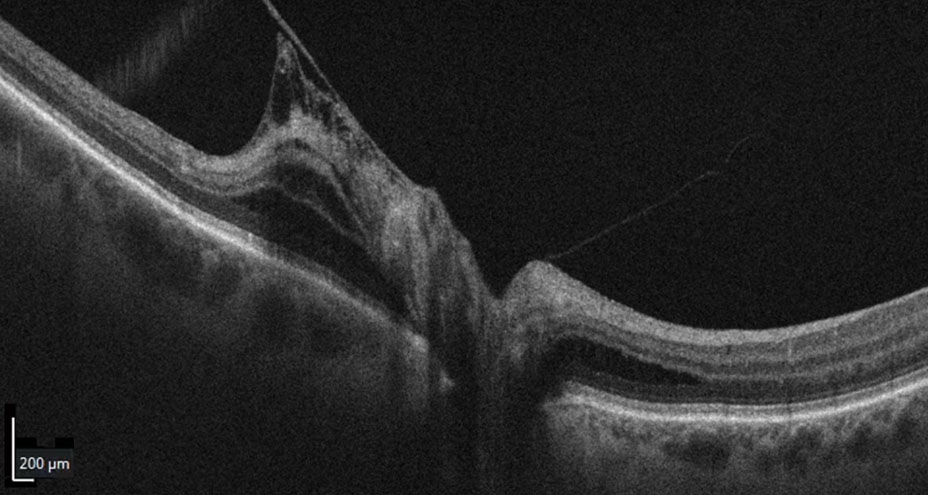
Given the unilateral disc hyperemia, vision changes, systemic vascular risk factors, and recent high-altitude exposure, initial consideration was given to a potential diagnosis of an incipient non-arteritic anterior ischemic optic neuropathy (NAION) [1] in the left eye. The mild asymmetry between eyes on exam and fundus imaging warranted optical coherence tomography (OCT) imaging. Optical coherence tomography of the left eye (Figure 2) reveals peripapillary adhesion and traction of the posterior hyaloid with schisis of the nerve fiber, ganglion, inner nuclear, and outer nuclear layers, without subretinal fluid, ultimately leading to a diagnosis of vitreomacular peri/papillary traction syndrome. Serological testing was performed and the patient’s complete blood count (CBC), basic metabolic panel (BMP), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), as well Syphilis, TB quantiferon, anti-neutrophil cytoplasmic antibodies (ANCA), Sjögren’s-syndrome-related antigen A [SSA (Ro)], Sjögren’s-syndrome-related antigen B [SSA (La)], and Bartonella were negative, whereas angiotensin-converting enzyme (ACE) was elevated (93 U/L). Recent exposure to high altitude, which is associated with hypoxia and transient alterations in microvascular perfusion [2],[3],[4], may represent a relevant contextual factor in the setting of tractional deformation of peripapillary vessels, although a causal relationship cannot be established. High altitudes can also increase the risk of developing a NAION.
The patient was referred to the retina service for vitreomacular traction (VMT). Pars plana vitrectomy was not recommended due to preserved visual function and lack of foveal involvement [5],[6], with additional concern for surgical release of vitreopapillary traction precipitating iatrogenic nerve fiber damage in eyes with small optic nerve cups, although this is controversial [7]. While the finding of vitreopapillary traction was severe, the patient was advised to follow up regularly for surveillance.
This case emphasizes the importance of considering a dilated exam to rule out alternative structural or anatomic abnormalities in patients presenting with presumed optic disc edema or hyperemia. Vitreomacular traction (VMT) typically occurs in patients with macular diseases such as diabetic retinopathy, diabetic macular edema, age-related macular degeneration, and inflammatory eye diseases. Over time, the vitreous gel undergoes age-related condensation, including liquefaction and loss of volume, leading to traction on retinal and papillary attachments. Signs associated with vitreous traction include intraretinal and subretinal fluid, as well as the development of an epiretinal membrane [8].
Conclusion
This case highlights an unusual presentation of vitreopapillary traction mimicking unilateral optic disc edema resulting in an anomalous optic nerve appearance. Awareness of this potential presentation is crucial for accurate differentiation and appropriate management. The patient continues to follow up regularly for monitoring of vitreopapillary traction with stable, preserved visual acuity.
REFERENCES
1.
Biousse V, Newman NJ. Ischemic optic neuropathies. N Engl J Med 2015;372(25):2428–36. [CrossRef]
[Pubmed]

2.
Baker J, Safarzadeh MA, Incognito AV, Jendzjowsky NG, Foster GE, Bird JD, et al. Functional optical coherence tomography at altitude: Retinal microvascular perfusion and retinal thickness at 3,800 meters. J Appl Physiol (1985) 2022;133(3):534–45. [CrossRef]
[Pubmed]
3.
De Abreu J, Paillisser A, Berquet F, Hogg S, Trucco E, Geiser MH, et al. Changes in retinal vasculature phenotype and choroidal blood flow at high altitude in healthy lowlanders. Invest Ophthalmol Vis Sci 2025;66(6):50. [CrossRef]
[Pubmed]
4.
Bosch MM, Barthelmes D, Merz TM, Bloch KE, Turk AJ, Hefti U, et al. High incidence of optic disc swelling at very high altitudes. Arch Ophthalmol 2008;126(5):644–50. [CrossRef]
[Pubmed]
5.
Bottós JM, Elizalde J, Rodrigues EB, Maia M. Current concepts in vitreomacular traction syndrome. Curr Opin Ophthalmol 2012;23(3):195–201. [CrossRef]
[Pubmed]
6.
Hikichi T, Yoshida A, Trempe CL. Course of vitreomacular traction syndrome. Am J Ophthalmol 1995;119(1):55–61. [CrossRef]
[Pubmed]
7.
Parsa CF, Hoyt WF. Nonarteritic anterior ischemic optic neuropathy (NAION): A misnomer. Rearranging pieces of a puzzle to reveal a nonischemic papillopathy caused by vitreous separation. Ophthalmology 2015;122(3):439–42. [CrossRef]
[Pubmed]
8.
Bottós J, Elizalde J, Arevalo JF, Rodrigues EB, Maia M. Vitreomacular traction syndrome. J Ophthalmic Vis Res 2012;7(2):148–61.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
John Abdelmalek - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Claire E Malley - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Andrew W Browne - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Lilangi S Ediriwickrema - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 John Abdelmalek et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.