 |
Case Report
Traumatic anterior capsule rupture in a patient with Alport syndrome without anterior lenticonus
1 Department of Ophthalmology, Dhahran Eye Specialist Hospital, Dhahran, Saudi Arabia
Address correspondence to:
Faisal A AlTahan
Al Naeim St, Dhahran,
Saudi Arabia
Message to Corresponding Author
Article ID: 100052Z17FA2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
AlTahan FA, AlRushoud M. Traumatic anterior capsule rupture in a patient with Alport syndrome without anterior lenticonus. J Case Rep Images Opthalmol 2026;9(1):11–14.ABSTRACT
Introduction: To report a rare case of traumatic anterior lens capsule rupture in a patient with Alport syndrome (AS) occurring in the absence of anterior lenticonus, and to highlight the clinical course, imaging findings, and surgical considerations associated with the inherent anterior capsule fragility of AS.
Case Report: A 24-year-old male with AS presented after blunt ocular trauma with glare and reduced vision in the right eye. Examination revealed an isolated anterior lens capsule defect without cataract formation or anterior lenticonus. Over short-term follow-up, the defect progressed with early cataract formation and anterior nuclear protrusion confirmed on anterior segment optical coherence tomography. The patient underwent femtosecond laser-assisted capsulotomy and phacoemulsification with toric posterior-chamber intraocular lens implantation (PCIOL). Surgery was uneventful, and postoperative visual acuity and visual quality improved with resolution of glare.
Conclusion: Patients with AS possess intrinsically fragile anterior lens capsules due to type IV collagen defects and may develop anterior capsule rupture even without anterior lenticonus. Blunt trauma can precipitate isolated capsule dehiscence with minimal initial cataract formation, Femtosecond laser-assisted capsulotomy may offer enhanced safety in these patients by reducing the risk of capsular extension during surgery.
Keywords: Alport syndrome, Anterior capsule rupture, Traumatic cataract
Introduction
Alport syndrome (AS) is a rare inherited basement membrane disorder characterized by progressive renal impairment, bilateral sensorineural hearing loss, and a variety of ocular manifestations that arise due to mutations in the genes encoding of type IV collagen (COL4A3, COL4A4, COL4A5) [1]. Anterior lenticonus, which is characterized by anterior protrusion of the lens, is considered a pathognomonic ocular sign in patients with AS. The anterior capsule of AS patients tends to be thinner and significantly more fragile compared to healthy populations. Recent studies have shown that the central anterior capsule thickness may be as thin as 3 µm [2]. This fragility contributes to the high susceptibility of the anterior capsule to rupture, which has been documented in previous cases to occur spontaneously [3],[4].
Case Report
A 24-year-old male with a known history of AS diagnosed at the age of two years due to hematuria with progressive bilateral sensorineural hearing loss, presented to our clinic one week after sustaining direct blunt ocular trauma to the right eye from a ball impact while participating in a sport event. He reported blurriness of vision and glare in the affected eye. On examination, uncorrected visual acuity (VA) was 20/30 in the right eye and 20/25 in the left eye. Intraocular pressures were 11 mmHg and 12 mmHg in the right and left eye respectively.
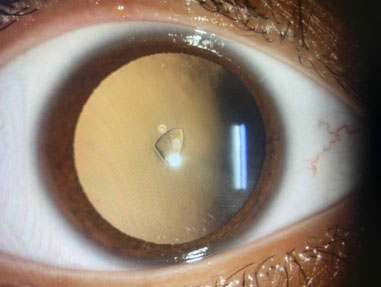
Anterior segment examination of the right eye revealed a quiet conjunctiva and sclera with no evidence of open-globe injury. The cornea was clear, and the anterior chamber was deep and well formed. Notably, an isolated small circular defect was observed in the anterior lens capsule without formation of cataract (Figure 1). There was no evidence of anterior lenticonus in both eyes and dilated fundus examination was unremarkable.
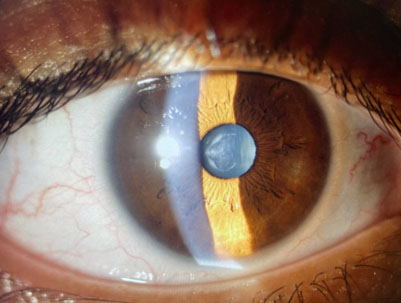
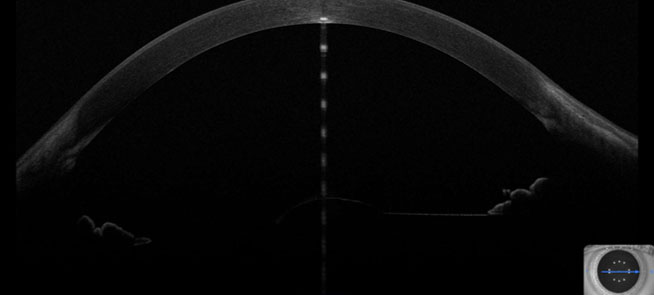
Subjective refraction showed plano sphere with –1.67 D of astigmatism at 167° in the right eye and plano sphere with –1.29 D astigmatism at 172° in the left eye. The patient was given a 2-week follow-up for reassessment. On follow-up visit, the patient reported increase in glare and repeated anterior segment examination revealed widening of the anterior capsule defect with an early cataract formation with faint protrusion of the nuclear material anteriorly toward the anterior chamber (Figure 2). Anterior segment-optical coherence tomography (AS-OCT) detailed the central anterior capsule defect along with faint nuclear protrusion into the anterior chamber in the right eye without the presence of an underlying anterior lenticonus (Figure 3). The decision to perform phacoemulsification with toric posterior-chamber intraocular lens (PCIOL) implantation was made. A femtosecond-assisted laser was utilized to perform a 5.0-mm capsulotomy using a selective laser to reduce the risk of capsule runout, as the anterior capsule appeared fragile. A +19.00 D toric PCIOL was implanted in the capsular bag.
On the first postoperative day, the patient’s visual acuity was 20/28 with a clear cornea, deep and quiet anterior chamber, and the PCIOL was well centered in the bag. Two weeks after surgery, at the subsequent follow-up visit, the patient reported significant improvement in vision, reaching 20/22 with resolution of the glare. After three months, the postoperative outcome was satisfactory with no complications. The patient was kept under close observation on a 6-month basis for routine ophthalmic assessment.
Discussion
The pathophysiology underlying these changes is attributed to mutations mainly in the COL4A5 gene, which leads to structural weaknesses not only in the glomerular basement membrane but also in other supporting tissues, including the lens capsule [5]. Understanding these structural alterations in the anterior lens capsule, even in patients without anterior lenticonus, is essential to provide optimal care with safe surgical outcomes.
Anterior capsule rupture can occur spontaneously or after trauma in patients with AS and is usually accompanied by a visually significant cataract with the presence of anterior lenticonus. In our case, the patient did not have any evidence of anterior lenticonus. However, pre-existing anterior capsule fragility was most likely present, as the blunt trauma resulted only in an anterior capsule rupture without any significant cataract formation or ocular surface injury at the initial visit. Although a rare occurrence, traumatic anterior capsule rupture in AS patients has been previously documented in the literature, with most cases exhibiting varying degrees of anterior lenticonus with cataract formation and nuclear material extrusion into the anterior chamber [6]. However, to the best of our knowledge, there has been no previous documentation of an anterior capsule rupture in the absence of anterior lenticonus in patients with AS.
As previously discussed, the anterior lens capsule in individuals with AS shows considerable thinning compared to typical structure and anatomy, with these patients often having only one-third of the normal capsular thickness. In a previous study conducted by Sonarkhan et al. in which the excised anterior capsule during phacoemulsification was sent for histological electron microscopy assessment, which showed multiple linear and irregular capsular dehiscences, several of which contained fibrillar and irregular electron-dense material along with vacuoles [7].
Another ultrastructural study by Bayar et al. in which 15 patients with AS who underwent phacoemulsification were reviewed. Electron microscopy assessment was done for those patients and revealed marked thinning of the capsule with numerous dehiscences, which aligns with previous studies in the literature [8].
Employing meticulous surgical techniques is crucial to managing the inherent risks associated with the fragile anterior capsule. Aslanzadeh et al. highlighted that, during phacoemulsification in patients with AS, the capsulorhexis demonstrates a tendency to slightly widen or run out [9]. In addition, particular consideration should be given to the perioperative setting in these patients, as intraoperative cooperation is likely to be suboptimal due to the frequently associated hearing impairment, making general anesthesia or meticulous communication strategies especially important.
In such cases, it is prudent to intervene in a timely manner to prevent further cataract formation or prolapse of lens material into the anterior chamber, which may trigger an inflammatory reaction, causing high intraocular pressure and uveitis, such as in cases of phacoantigenic glaucoma. In addition, we found that utilizing a laser-assisted capsulorhexis device intraoperatively helps maintain anterior capsule integrity and reduces the risk of extension compared to manual capsulorhexis.
Conclusion
Patients with AS, even in the absence of anterior lenticonus, have a high susceptibility to anterior capsule rupture following blunt trauma due to the fragile nature of their anterior capsule. Careful preoperative assessment and early surgical planning are essential to prevent complications and achieve optimal visual outcomes. Femtosecond-assisted laser capsulotomy can be a safe and reliable method of performing anterior capsulotomy particularly in such cases.
REFERENCES
1.
Ohkubo S, Takeda H, Higashide T, Ito M, Sakurai M, Shirao Y. Immunohistochemical and molecular genetic evidence for type IV collagen alpha5 chain abnormality in the anterior lenticonus associated with Alport syndrome. Arch Ophthalmol 2003;121(6):846–50. [CrossRef]
[Pubmed]

2.
Lohchab M, Arora R. Bilateral spontaneous lens capsule rupture in Alport’s syndrome. Indian J Ophthalmol 2019;67(3):406. [CrossRef]
[Pubmed]
3.
Banayot RG, Sargent N. Bilateral lens capsule rupture in a patient with previously undiagnosed Alport’s syndrome. Ophthalmol J 2021;6:57–60. [CrossRef]
4.
Chaurasia S, Garg P. Bilateral spontaneous rupture of the anterior capsule. J Cataract Refract Surg 2008;34(8):1413–5. [CrossRef]
[Pubmed]
5.
Tiwari US, Aishwarya A, Kujur R. Bilateral combined anterior and posterior lenticonus in Alport’s syndrome. Rom J Ophthalmol 2018;62(3):228–30.
[Pubmed]
6.
Gouws D, van der Westhuizen DP, Stuart KV. Bilateral anterior lens capsule rupture in Alport syndrome: Case series and literature review. Digit J Ophthalmol 2024;30(3):55–9. [CrossRef]
[Pubmed]
7.
Sonarkhan S, Ramappa M, Chaurasia S, Mulay K. Bilateral anterior lenticonus in a case of Alport syndrome: A clinical and histopathological correlation after successful clear lens extraction. BMJ Case Rep 2014;2014:bcr2013202036. [CrossRef]
[Pubmed]
8.
Bayar SA, Pinarci EY, Karabay G, Akman A, Oto S, Yilmaz G. Clear lens phacoemulsification in Alport syndrome: Refractive results and electron microscopic analysis of the anterior lens capsule. Eur J Ophthalmol 2014;24(3):345–51. [CrossRef]
[Pubmed]
9.
Aslanzadeh GA, Gharabaghi D, Naderi N. Clear lens phacoemulsification in the anterior lenticonus due to Alport syndrome: Two case reports. J Med Case Rep 2008;2:178. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Faisal A AlTahan - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Muath AlRushoud - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Faisal A AlTahan et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



