 |
Clinical Image
Mycosis fungoides with large cell transformation of the upper eyelid
1 Orbital, Plastics and Lacrimal (OPAL) Unit, Royal Victorian Eye and Ear Hospital, East Melbourne, Victoria, Australia
2 Department of Anatomical Pathology, St Vincent’s Hospital, Fitzroy, Victoria, Australia
3 Department of Surgery, Royal Melbourne Hospital, University of Melbourne, Parkville, Victoria, Australia
Address correspondence to:
Callum Gin
Orbital, Plastics and Lacrimal (OPAL) Unit, Royal Victorian Eye and Ear Hospital, East Melbourne, Victoria,
Australia
Message to Corresponding Author
Article ID: 100038Z17CG2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Gin C, Hyer J, Mckelvie P, Hardy TG. Mycosis fungoides with large cell transformation of the upper eyelid. J Case Rep Images Opthalmol 2023;6(2):1–3.ABSTRACT
No Abstract
Keywords: Cutaneous lymphoma, Mycosis fungoides, Ocular oncology
Case Report
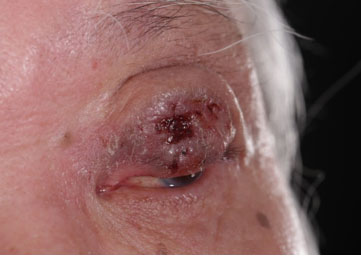
An 86-year-old man was referred to the emergency department with two months of an enlarging urticarial lesion of his left upper eyelid (LUL). Past medical history included long standing reduced right vision and chronic dermatitis. He had no history of cancer, smoking, or alcohol consumption.
Clinically, there was a 30×19 mm LUL lesion extending beyond the upper tarsus with ulceration, keratinization, and madarosis (Figure 1). There was no gaze restriction. Trigeminal nerve sensation was intact. There was erythematous plaque involving the forehead.
Best corrected visual acuity was 6/120 in the right eye and 6/12 in the left. Intraocular pressure was normal bilaterally. Pupil, anterior segment, and fundal examination were unremarkable.
Histologically, the forehead plaque was consistent with mycosis fungoides (MFs). There was epidermotropism and folliculotropism by small-medium lymphoid cells forming Pautrier micro-abscesses in the follicular epithelium. Immunohistochemistry showed CD2+, CD3+, CD4+, CD5+, CD7–, CD8–, CD30+ in a minor subset (10%), T-cell intracellular antigen-1, granzyme B−. Less than 25% of the cells were large.
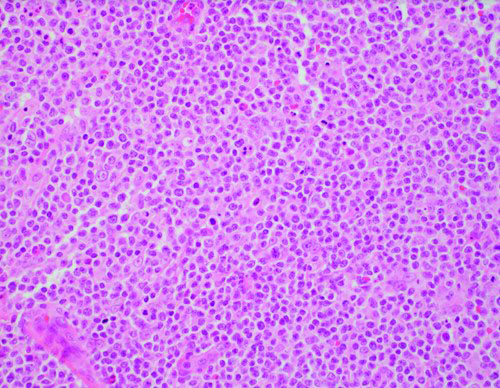
The LUL lesions were consistent with large cell transformation of MF. Histology showed diffuse infiltration of large atypical lymphoid cells from the basal epidermis to the deep margin in the deep dermis (Figure 2). There was focal epidermotropism with follicular mucinosis. Immunohistochemistry of the large cells showed CD3+, CD2+, CD4+, CD8−, CD30+, ALK−, P63−, granzyme-B+ in subset.
Discussion
Mycosis fungoide is the most common cutaneous T-cell lymphoma [1]. It commonly affects males (ratio of 2:1 male to female) typically aged 45–60 years [1]. Clinical presentation is varied. Early stages present with limited patches and plaques, while later stages involve the lymph nodes and viscera. It may be misdiagnosed as chronic contact or atopic dermatitis. Extra-ocular manifestations of MF are seen in 2% of all MF cases [2]. Ophthalmic findings predominantly affect the eyelid and ocular surface, most commonly associated with seborrheic blepharoconjunctivitis [2]. Pruritis is a common accompanying symptom [1]. Large cell transformation of MF can occur at any stage and is associated with disease progression and poor outcomes.
Conclusion
This demonstrates the complexity of diagnosing MF. There are a range of possible differential diagnoses. An ophthalmologist should retain diagnostic suspicion in a patient with a history of widespread chronic pruritis alongside other skin lesions.
REFERENCES
1.
Jawed SI, Myskowski PL, Horwitz S, Moskowitz A, Querfeld C. Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome): Part I. Diagnosis: Clinical and histopathologic features and new molecular and biologic markers. J Am Acad Dermatol 2014;70(2):205.e1–16. [CrossRef]
[Pubmed]

2.
Colossi CG, Mondadori J, Barreto PKM, Valença FM, Duquia R, Vilela MAP. Mycosis fungoides: Analysis of ophthalmologic findings in a series of cases. Case Rep Dermatol Med 2019;2019:2380598. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
We are grateful for the guidance AM has provided.
Author ContributionsCallum Gin - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jonathan Hyer - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Penny Mckelvie - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Thomas G Hardy - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Callum Gin et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



