 |
Clinical Image
Large conjunctival epithelial inclusion cyst following scleral tunnel incision for cataract surgery
1 Resident, Department of Ophthalmology, Massachusetts Eye and Ear Infirmary, Harvard Medical School, Boston, MA, USA
2 Assistant Professor of Ophthalmology, Department of Ophthalmology, Massachusetts Eye and Ear Infirmary, Harvard Medical School, Boston, MA, USA
Address correspondence to:
Emma C Davies
MD, Department of Ophthalmology, Massachusetts Eye and Ear Infirmary, Harvard Medical School, 243 Charles Street, Boston, MA 02114,
USA
Message to Corresponding Author
Article ID: 100026Z17YB2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Bian Y, Stagner AM, Davies EC. Large conjunctival epithelial inclusion cyst following scleral tunnel incision for cataract surgery. J Case Rep Images Opthalmol 2022;5:100026Z17YB2022.ABSTRACT
No Abstract
Keywords: Conjunctival cyst, Phacoemulsification, Scleral tunnel
Case Report
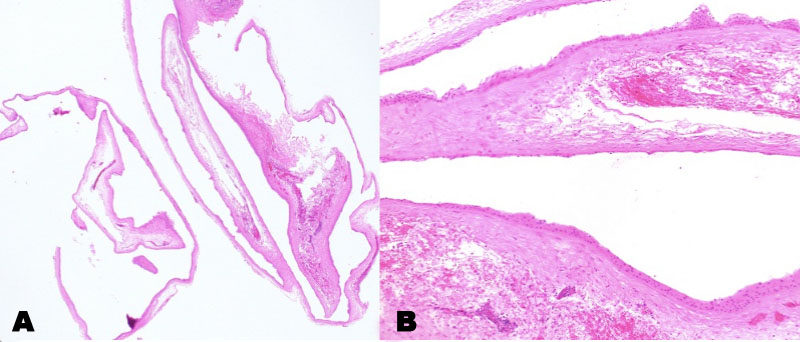
A 79-year-old man underwent right eye phacoemulsification cataract extraction and intraocular lens implantation. Intraoperatively, a superior, fornix-based conjunctival peritomy was created with blunt Wescott scissors for a scleral tunnel incision made 1.5 mm from the limbus and 3 mm in length. At the conclusion of the case, the conjunctiva was closed with cautery. We do not typically use scleral tunnel incisions for cataract surgery but do in certain cases such as Fuchs corneal dystrophy (to reduce corneal endothelial decompensation), history of LASIK (to reduce risk of flap disruption), and shallow anterior chamber (to reduce endothelial decompensation). At this patient’s one-year postoperative follow-up, his examination was notable for a well-circumscribed, thin-walled, cystic conjunctival lesion at the location of the previous superior peritomy which by the two-year postoperative visit had increased in size to 8 mm by 9 mm (Figure 1A). Vision was 20/25 OD (left eye) and 20/30 OS (left eye), intraocular pressure was 17 mmHg OD and 15 mmHg OS, and his dilated eye examination was unremarkable OU. Given the prominent cystic lesion with associated right upper eyelid ptosis, the patient elected for surgical removal. Intraoperatively, blunt Wescott scissors were used to create a superior conjunctival peritomy and carefully dissect conjunctival tissue from the cyst wall, with care taken to not rupture the cyst. A Crescent blade was used to separate the conjunctival tissue from the edges of the cyst, and the cyst was removed in its entirety with an intact capsule. The superior conjunctiva was repositioned at the limbus and held in place with Tisseel (fibrin sealant). Histopathologic examination revealed a cystic cavity lined by nonkeratinized, stratified squamous epithelium, ranging in thickness from 2 to approximately 8 cell layers. Metaplastic changes were present including focal surface glycogenation; goblet cells were not conspicuous. The squamous lining was associated with dense subepithelial fibrosis. The findings were consistent with a secondary conjunctival inclusion cyst (Figure 2A and Figure 2B). At two months, the patient displayed a well-healed superior conjunctival incision and no evidence of cyst recurrence (Figure 1B).

Discussion
Conjunctival inclusion cysts are the most common cystic lesion of the conjunctiva, making up 80% of conjunctival cysts [1],[2]. Conjunctival cysts can be either primary or develop secondarily. The most common cause of acquired conjunctival cyst is following ophthalmic surgery or penetrating trauma. Conjunctival incision allows for subsequent invagination and implantation of conjunctival epithelial cells [1]. After implantation, two layers of epithelium proliferate and a central cavity develops between them forming a cyst [3]. The majority of postoperative conjunctival inclusion cysts after cataract surgery have been reported following extracapsular cataract extraction and more recently small incision cataract surgery [1],[4]. To our knowledge, the development of a conjunctival inclusion cyst after phacoemulsification cataract surgery has only been rarely described in the literature [3]. Similar to our case, the patient described by Williams et al. also underwent a conjunctival peritomy and scleral tunnel incision [3]. Likely the prevalence of clear corneal incisions as the preferred method of wound construction in phacoemulsification cataract surgery has decreased the risk of conjunctival manipulation and development of conjunctival inclusion cysts. Conjunctival inclusion cysts are usually asymptomatic but if large can be cosmetically unacceptable, cause foreign body sensation and dry eye syndrome, and result in eyelid ptosis and affect eye movement [1]. Treatment for symptomatic conjunctival inclusion cysts is most commonly complete surgical removal, which also allows for definitive histopathologic diagnosis. Recurrence of the cyst is the main postoperative concern. Complete and intact removal of the cyst can significantly reduce this risk. Other treatment modalities have been reported including needle drainage and thermal cautery, but long-term data on rate of cyst recurrence following these interventions is lacking [5].
Conclusion
Conjunctival inclusion cysts can develop after scleral tunnel incisions for phacoemulsification cataract surgery. Complete surgical removal is the definitive treatment for symptomatic conjunctival inclusion cysts.
REFERENCES
1.
Thatte S, Jain J, Kinger M, Palod S, Wadhva J, Vishnoi A. Clinical study of histologically proven conjunctival cysts. Saudi J Ophthalmol 2015;29(2):109–15. [CrossRef]
[Pubmed]

2.
Nath K, Gogi R, Zaidi N, Johri A. Cystic lesions of conjunctiva (a clinicopathological study). Indian J Ophthalmol 1983;31(1):1–4.
[Pubmed]
3.
Williams BJ, Durcan FJ, Mamalis N, Veiga J. Conjunctival epithelial inclusion cyst. Arch Ophthalmol 1997;115(6):816–7. [CrossRef]
[Pubmed]
4.
Narayanappa S, Dayananda S, Dakshayini M, Gangasagara SB, Prabhakaran VC. Conjunctival inclusion cysts following small incision cataract surgery. Indian J Ophthalmol 2010;58(5):423–5. [CrossRef]
[Pubmed]
5.
Hawkins AS, Hamming NA. Thermal cautery as a treatment for conjunctival inclusion cyst after strabismus surgery. J AAPOS 2001;5(1):48–9. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Yandong Bian - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Anna M Stagner - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Emma C Davies - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 Yandong Bian et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



